External ear reconstruction
This is considered one of the most complex procedures in plastic surgery. It is a lengthy and multi-stage process that requires precise planning and close cooperation between the patient and Dr. Slosser. This type of surgery is performed on three main groups of patients:
- Patients born with ear malformations (anotia or microtia);
- Patients who have lost the shape of their ears due to trauma, cancer, or other diseases;
- Patients who have undergone unsuccessful ear reconstruction surgery.

Today, there are three conceptually different options for reconstruction:
- Reconstruction using the patient's own tissue;
- Reconstruction using an ear implant;
- Non-surgical reconstruction using an ear prosthesis to hide the defect;
Of course, each technique has its advantages and disadvantages. At our clinic in Kyiv, we offer ear reconstruction using the patient's own tissue (rib cartilage). This technique allows us to achieve the most natural ear shape and long-lasting results. The advantage of using ear implants is a significant reduction in the duration of surgery and less tissue trauma, since no rib cartilage is removed. On the other hand, most surgeons refuse to use this technique because the use of implants in reconstruction is accompanied by a significant risk of inflammation and extrusion (falling out) even with minimal trauma. It is precisely because of its low reliability that we do not use this technique. The use of prostheses also does not provide a high level of patient satisfaction, as the prosthesis cannot provide natural shapes and colors and requires daily care. The use of prostheses in children is recommended from the age of 8.
Ear reconstruction in microtia and anotia
What is microtia?
Microtia is a congenital deformity of the outer ear. Translated from Greek, it means “small ear.” Incidence: approximately one case in every 6,000 newborns, 10% of children have bilateral pathology. More severe degrees of microtia, characterized by narrowing or atresia of the ear canal, are also accompanied by hearing impairment. The cause of microtia is not fully understood. As a rule, it is not genetically inherited, with the exception of Treacher-Collins syndrome. It is also worth noting that 20 to 60% of children with this pathology have concomitant pathologies and require additional examination. Most often, microtia is combined with malformation of the lower jaw and zygomatic arches. Congenital ear abnormalities are the most common reason for ear reconstruction.
Today, there are several ways to classify these defects, but ear abnormalities are most often classified as follows:
Type I microtia: the ear is smaller in size, but all structural parts of the ear and the external auditory canal are present;
Type II microtia: the upper part of the ear is usually absent and there is a projection deficit. The auditory canal is usually stenosed or there is atresia of the auditory canal;
Type III microtia: complete absence of the auditory canal and presence of only an underdeveloped earlobe;
Microtia type IV (Anotia): Complete absence of the auditory canal and auricle.
Before planning surgery, the following examinations must be performed:
Audiological testing to assess the sound threshold and determine possible conductive hearing loss
CT scan to visualize the temporal bones and structures of the inner ear and then create a 3D model of the ear
MRI – needed in some cases to visualize the course of the facial nerve and temporal vessels, as their normal anatomy is often disrupted in microtia

To get the best result, the surgeon should keep in mind 3 basic principles:
- Correct positioning of the future ear
- Use of tissues with good blood supply
- Creation of an anatomically correct cartilage framework in accordance with the patient's proportions
How is the surgical procedure performed?
Treatment varies depending on the stage.
In type 1 microtia, it is usually not necessary to harvest rib cartilage; the surgeon performs reconstruction using local tissues. The correct anatomical shape is created by remodeling the existing cartilage. This operation can be performed under local anesthesia.

In type 2 microtia, the surgeon usually removes only the free (floating) rib and then forms the missing structures. In some cases, this requires several surgical procedures. The duration of the surgery is 3-4 hours, followed by observation in the clinic for up to 2 days.
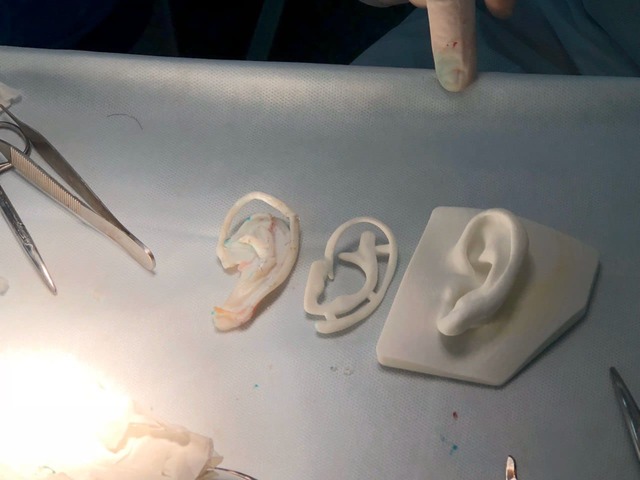
In type 3-4 microtia, reconstruction is performed in two stages. During the first stage, Dr. Slosser carefully marks and forms a “pocket” for the modeled cartilage, after which the surgeon removes the rib cartilage and models the framework of the future ear according to the previously determined dimensions. The surgeon then inserts the framework into the previously determined location and sutures the tissues. This surgical procedure lasts 4-5 hours and requires a hospital stay of about 2-3 days.

The second stage of reconstruction is planned no earlier than 6 months later. During the operation, the framework is detached from the surface to create a natural projection of the ear. The back of the ear is covered with a skin flap. This operation lasts 2-3 hours and requires the patient to stay in the clinic for up to 2 days.
Ear reconstruction due to trauma or cancer:
The most common types of ear injuries are:
- Animal and human bites
- Mechanical trauma
- Thermal trauma (burns and frostbite)
Cancer of the outer ear is rare; ear reconstruction is more often performed as a result of the removal of neoplasms from the surrounding areas.
It should be noted that there is no universal option for reconstruction in these cases. Dr. Slosser plans surgical intervention based on the amount of tissue lost and the mechanism of injury. However, the principles of reconstruction remain similar to those used in the reconstruction of congenital ear defects. Small wounds with minor tissue loss can be repaired by manipulating only the affected ear or taking extra tissue from the other ear. For big defects or when the ear is totally missing, the surgery is the same as for microtia types 3 and 4. A factor that significantly complicates surgery is that the surgeon is working with damaged and possibly infected tissue with impaired blood supply. This is in contrast to the reconstruction of congenital anomalies, where the tissue is intact at the time of reconstruction.
Frequently asked questions:
What are the most common complications of ear reconstruction?
Hematoma is a rare complication, occurring in about 0.5% of cases, and can be resolved with adequate drainage.
Wound infection can occur in both the early and late postoperative period, occurring in about 1% of patients. If symptoms of infection or inflammation (pain, fever, redness, discharge in the ear area) are detected, you should immediately consult a doctor.
Necrosis of the skin flap: depends on many factors, but the correct surgical technique and the use of gentle dressings can minimize this complication.
Resorption (dissolution) of cartilage occurs due to insufficient blood supply and a deficiency of substances necessary for cartilage function. As a result, patients may subsequently complain of a lack of the desired ear contour.
Is specific rehabilitation necessary after reconstruction?
No, proper care of the postoperative wound, minimization of trauma, and wearing a protective bandage will allow you to achieve optimal results.
Will my child's hearing improve after surgery?
In cases of stenosis and atresia of the auditory canal, patients usually notice an improvement in hearing after its reconstruction.
Can I be a cartilage donor for my child?
Theoretically, yes, but this has no practical application. If foreign biological material is implanted, your child will have to take immunosuppressive therapy for the rest of their life. This has significantly more negative effects than the additional trauma associated with cartilage tissue removal.
How can facial asymmetry in microtia be corrected?
In cases of significant facial asymmetry, there are several options for correction: the use of implants, the injection of the patient's own fat cells (lipofilling), or fillers.
What scar remains after rib cartilage is harvested?
It depends on the amount of material needed for harvesting, but usually a scar about 10 cm long and 1-3 mm wide remains after harvesting.
What types of ear implants are available?
The most commonly used implants are MEDPOR porous polyethylene implants, but implants made of solid silicone are also used.
At what age should children with microtia undergo surgery?
We recommend surgery at the age of 6, which allows the final result to be achieved before the child starts school. This helps the child avoid possible complexes and problems related to social interaction.
Does my child need ear reconstruction if they do not see a problem with it and are completely happy?
If the child does not experience any discomfort, we recommend refraining from surgery. Talking to families with similar experiences may also help you make a decision. However, if the child develops complexes about this, we recommend consulting a psychologist and deciding on further reconstruction.

Honored Doctor of Ukraine, Head of the Plastic Surgery Center
FAQ
In short, pain is manageable. Severe pain after surgery today is the exception rather than the norm. Modern anesthesia, pain management, and recovery protocols make the first days much easier than most patients expect. Most often, discomfort is felt as pressure or tightness. However, it is important to understand that complete absence of sensation is an unrealistic expectation. My position is clear: if a person is afraid of any discomfort, it is better to postpone surgery. The decision must be conscious and well considered.
No. Rehabilitation is part of the surgery, not a separate stage afterward. It is during the recovery period that the final result is formed, tissues stabilize, and the risk of complications decreases. Without proper rehabilitation, even a technically perfect operation may produce a weak outcome. There are procedures with an easier recovery (for example, “weekend lifts”), but surgery without rehabilitation does not exist.
The final result does not appear immediately. It develops gradually over time. Swelling, tissue firmness, and sensations change step by step. During the first weeks, the result is definitely not final, and this is completely normal. The timeline depends on the treated area, the extent of surgery, and individual characteristics of the body. Plastic surgery does not tolerate haste. A good result takes time.
It depends primarily on the type of work you do, not only on the surgery itself. After some procedures, it is possible to return to work within a few days (for example, after “weekend lifts”), while others require weeks of recovery. It is important to consider not only how you feel, but also the safety of the healing process. Returning to activity earlier than recommended increases the risk of complications. It is better to return later than to deal with the consequences of rushing.
Yes, scars always remain. This is part of the natural healing process. However, their appearance changes over time: they become lighter, softer, and less noticeable. Their location and proper care play a crucial role. Careful planning and patience are essential.
When the risks outweigh the benefits, or when the decision is driven by emotions. I refuse if I see that the body is not ready, expectations are unrealistic, or the person does not understand the recovery process. Refusal is also part of treatment. Safety is more important than any desire.
Yes, and it has a significant impact on the outcome. Honest answers, a list of questions, and a willingness to listen save time and help you make the right decision. A consultation is a diagnosis, not a sales pitch. A good consultation is half the success.

Calculate the cost of the operation: Ear reconstruction
Leave your details and we will contact you for an accurate assessment of the operation
Materials on the topic
Операция по реконструкции мочки уха
Целью операции является создание естественной формы мочки уха, которая будет соответствовать форме вашего лица, и повысит вашу самооценку. В этой статье я расскажу, чего ожидать от операции по восстановлению мочки уха и как вы можете к ней подготовиться.

Why Ukrainians turn to plastic surgeons – a survey of Dmytro Slosser's audience
Last week, I conducted a brief survey among my followers on Instagram using the Stories feature. Each question received a different number of responses, but on average, approximately 400 respondents participated. The purpose of this survey was quite simple: to understand what motivates people to undergo cosmetic surgery today. The results confirmed my own observations.
