Facial Correction After Rapid Weight Loss: Restoration of Lost Volume and Skin Lifting
I am increasingly working with patients who have achieved significant weight loss—on their own, after bariatric surgery, or while taking popular medications (in particular, such as Ozempic). And almost invariably, along with a new body they notice an unexpected effect: the face appears older than it did before the weight loss. Unfortunately, these are not isolated cases, but a predictable anatomical process.
Why the face “ages” after weight loss
Rapid weight loss is accompanied not only by a reduction of fat tissue in the body, but also by a significant loss of volume in the midface and upper facial thirds. According to studies, cheek fat compartments can decrease by up to 70% after substantial weight loss, leading to hollow cheeks, more pronounced nasolabial folds, and an overall “depleted” appearance.
Moreover, fat in the deeper facial structures plays a supportive role. Its loss triggers a cascade of structural changes: tissues descend, contours become less defined, and the skin becomes less taut. When combined with age-related decline in elasticity, this results in a typical clinical picture: a combination of volume deficiency and soft tissue ptosis (sagging).
The key principle of correction: restore volume and lift tissues
Modern aesthetic surgery has long moved beyond the concept of simply “tightening the skin.” Today, we approach the face as a three-dimensional structure, where it is critical to restore lost volume and structural support.
The optimal strategy is almost always combined and includes:
- restoration of volume (fat grafting, fillers, biostimulators);
- lifting procedures (surgical or minimally invasive);
- improvement of skin quality (energy-based devices, injectable regenerative techniques).
It is precisely this combination of approaches that provides a natural aesthetic result, rather than an over-tightened, mask-like appearance.
Volume restoration: the foundation of rejuvenation
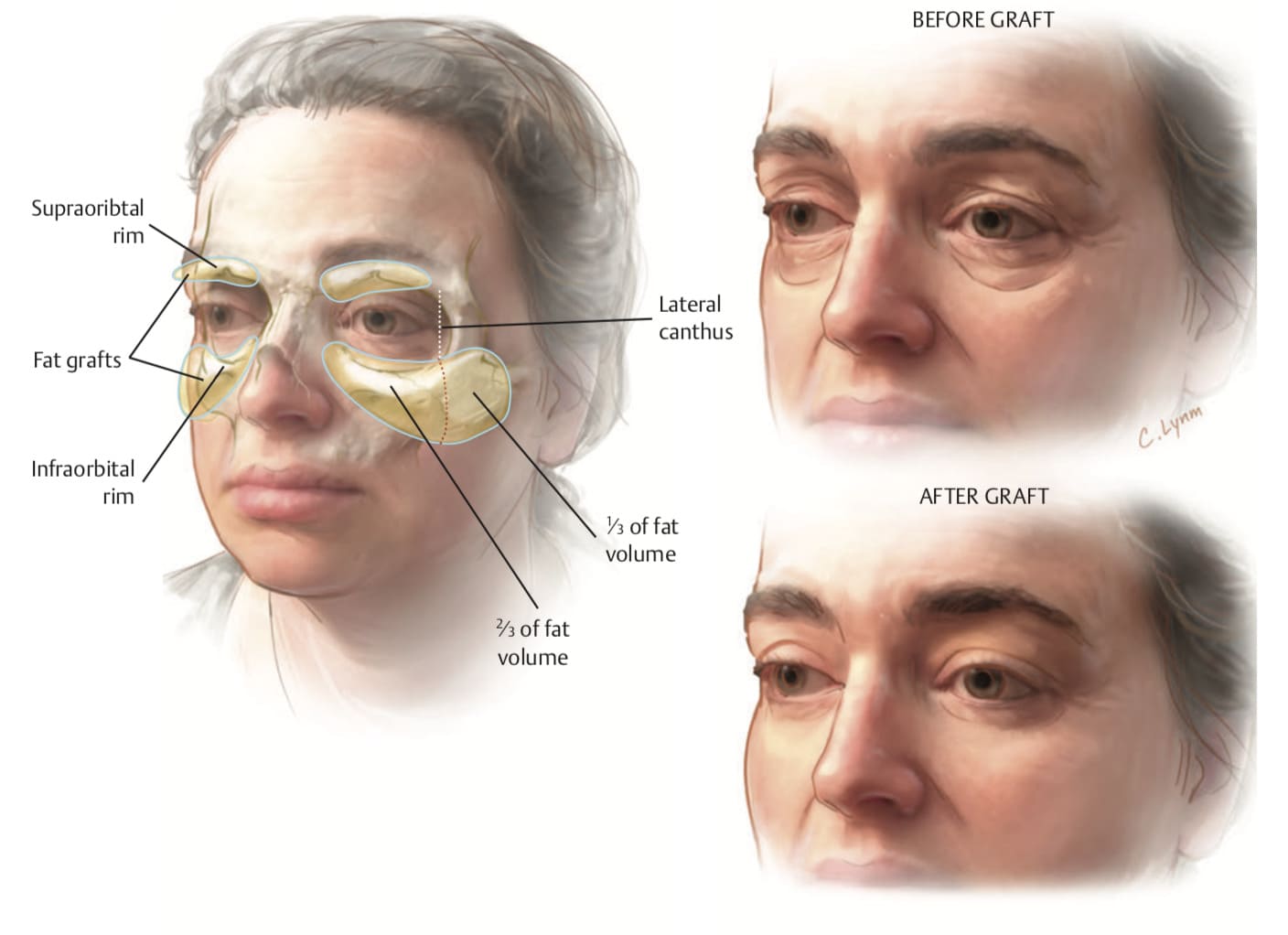
The most physiological method is autologous fat grafting—that is, the transfer of the patient’s own fat. This procedure restores not only volume, but also improves the quality of facial tissues.
According to research, fat graft survival can range from 26% to 83%, which explains why repeat procedures may sometimes be necessary. It is important to understand that transferred fat behaves like normal adipose tissue and may decrease with further weight loss. Therefore, patients should seek surgical correction once their weight has stabilized and is appropriate for their body composition.
In clinical practice, I often combine fat grafting with fillers. This “layered” approach allows us to create foundational volume while precisely refining delicate areas such as the under-eye region or the lip contour.
Lifting: when volume alone is not enough
If the skin has significantly lost its elasticity, volume restoration alone is not sufficient to fully address the problem. In such cases, lifting procedures become necessary.
Modern techniques, particularly the deep plane facelift, address not only the skin but also the deeper facial structures, allowing for a natural result without the appearance of excessive tightness. This approach provides a longer-lasting and anatomically sound outcome. A delicate lift is often combined with fat grafting, as even perfectly repositioned tissues can appear flat without adequate volume.
I would like to emphasize again: if a patient continues to lose weight after surgery, this may lead to further volume loss and partial regression of the result. Therefore, stable weight is an essential condition for a predictable outcome.
Minimally invasive alternatives to surgery
Surgical intervention is not always the optimal solution—sometimes there are medical contraindications, or the patient may not be psychologically ready for surgery. In such cases, we opt for a gradual, more conservative correction strategy:
- injectable fillers (hyaluronic acid);
- biostimulators (such as poly-L-lactic acid);
- energy-based treatments (radiofrequency, ultrasound).
These methods do not replace a full surgical lift in cases of pronounced ptosis, but they can improve skin quality, partially restore lost volume, and delay the need for more invasive procedures.
The importance of an individualized approach
In every case, in my opinion, an individualized approach is essential. Younger patients after weight loss often require only volume restoration—fat grafting and targeted filler injections. Patients aged 40+ typically need a combined approach (fat grafting together with a delicate lift). After significant weight loss (20–30 kg or more), a classic facelift is almost always indicated.
In most cases, my goal is not to “redo” the face, but to restore its natural proportions and volumes as they were before weight loss—only in a more harmonious and refined form.
Conclusion
Rapid weight loss changes the face no less than the body. These changes are not only aesthetic, but also anatomical. Effective correction is always based on two key principles: restoring volume and properly lifting the tissues. Only their combination allows for a natural result without obvious signs of surgical intervention.

Honored Doctor of Ukraine, Head of the Plastic Surgery Center
Contact me
Plastic surgeon
Ukraine, Kyiv, Shchekavytska St., 9a
(Clinic "Nove Tilo")
